الأسماء في صفحات التنقل
Brugia malayi ist ein tropischer Fadenwurm aus der Gruppe der Filarien. Er parasitiert beim Menschen und kann eine lymphatische Filariose und das Krankheitsbild der Elephantiasis verursachen.
Die adulten Würmer weisen die fadenwurmtypische längliche Struktur auf. Sie werden bis zu 2,5 cm (Männchen) bzw. 6 cm (Weibchen) lang[1].
Die Larven (Mikrofilarien, Larve 3) haben eine Größe von 200–300 µm und besitzen eine Hülle, die sich bereits über dem Ei findet und erst im Verdauungstrakt des infizierten Insekts aufgelöst wird. In dieser Form zirkulieren sie auch im menschlichen Blutkreislauf.[1]
Brugia malayi ist eine Tropenkrankheit, deren Verbreitungsgebiet in Südostasien liegt. Der Besiedelungsschwerpunkt liegt in Indien und China, andere betroffene Länder sind Indonesien, Thailand, Malaysia, die Philippinen und Vietnam[2].
Die Übertragung erfolgt durch Mücken der Arten Aedes, Culex, Anopheles und Mansonia.
Die adulten Filarien sitzen in den Lymphgefäßen, dort werden behüllte Mikrofilarien (über ein kurzes Ei Stadium) gebildet. Die Mikrofilarien – insbesondere jene aus Infektionen im Bereich offener Sumpfgebiete und Reisfelder – unterliegen einem Tagesrhythmus: Nachts werden sie im Blut verteilt und können so von Blut saugenden Insekten verbreitet werden; tagsüber reichern sie sich – als Folge des erhöhten Sauerstoffgehalts – in den kleinen Gefäßen der Lunge an.[3] Die größte Anzahl an Mikrofilarien ist im Blut zwischen Mitternacht und 2 Uhr früh nachweisbar.[4] In Bruchwäldern können jedoch auch Varianten vorkommen, die tagsüber im Blut verbreitet werden.
Im Verdauungssystem der Mücken löst sich die Hülle um die Mikrofilarien auf. Mithilfe einer Chitinaseaktivität können sie den Mitteldarm verlassen und sich im Thorax festsetzen. Dort entwickelt sich die L1 (Larve 1). Aus der L1 geht dann die L3 (Larve 3) hervor, die sich in der Speicheldrüse des Moskitos ansiedelt. Die Anzahl der Mikrofilarien, die das L3 Stadium im Insekt erreichen, ist sehr gering, daher reicht für die Infektion des Wirbeltierwirts (Mensch, Hauskatze etc.) ein einmaliger Stich nicht aus. Zudem entwickeln sich nur rund 10 % der L3 zum adulten Wurm, der sich in den Lymphgefäßen festsetzen kann.[5] Die Entwicklung infektiöser Larven in den Mücken erfordert hohe Temperaturen und Luftfeuchtigkeit. Nach einer Infektion siedeln sich die Filarien in Lymphbahnen an. Die Adultwürmer setzen nach etwa 3 Monaten Mikrofilarien ab. Über Aufnahme der Mikrofilarien durch einen erneuten Mückenstich schließt sich der Kreis. Die erwachsenen Würmer können 5 bis 15 Jahre im Wirt überleben.
Brugia malayi wurde erstmals 1927 von Lichtenstein und Brug innerhalb der Filarien abgegrenzt und als Filaria malayi beschrieben. Zuvor wurden sie als aufgrund der Ähnlichkeit zu Wuchereria bancrofti gezählt[6]. Diese Abgrenzung basierte auf den Mikrofilarien (dem Larvenstadium) der Fadenwürmer. Allgemeine Anerkennung fand diese Hypothese erst, als Rao und Maplestone in den 1940er Jahren zwei Exemplare des Adulten Wurmes in Indien fanden, der sich von Wuchereria bancrofti unterschied. Sie beschrieben die neue Art als Wuchereria malay[7].
Die heutige Einteilung in die zwei Gattungen Wuchereria und Brugia stammt vom Parasitologen J. S. Buckley.[4]
Brugia malayi ist ein tropischer Fadenwurm aus der Gruppe der Filarien. Er parasitiert beim Menschen und kann eine lymphatische Filariose und das Krankheitsbild der Elephantiasis verursachen.
Brugia malayi is a filarial (arthropod-borne) nematode (roundworm), one of the three causative agents of lymphatic filariasis in humans. Lymphatic filariasis, also known as elephantiasis, is a condition characterized by swelling of the lower limbs. The two other filarial causes of lymphatic filariasis are Wuchereria bancrofti and Brugia timori, which both differ from B. malayi morphologically, symptomatically, and in geographical extent.[1]
B. malayi is transmitted by Mansonia mosquitoes and is restricted to South and Southeast Asia. It is one of the tropical diseases targeted for elimination by the year 2020 by the World Health Organization, which has spurred vaccine and drug development, as well as new methods of vector control.
B. malayi is one of the causative agents of lymphatic filariasis, a condition marked by infection and swelling of the lymphatic system. The disease is primarily caused by the presence of worms in the lymphatic vessels and the resulting inflammatory response of the host. Signs of infection are typically consistent with those seen in Bancroftian filariasis—fever, lymphadenitis, lymphangitis, lymphedema, and secondary bacterial infection—with a few exceptions.
Lymphadenitis, the swelling of the lymph nodes, is a commonly recognized symptom of many diseases. It is an early manifestation of filariasis, usually occurs in the inguinal area during B. malayi infection and can occur before the worms mature.[2]
Lymphangitis is the inflammation of the lymphatic vessels in response to infection. It occurs early in the course of infection in response to worm development, molting, death, or bacterial and fungal infection. The affected lymphatic vessels become distended and tender, and the overlying skin becomes erythematous and hot. Abscess formation and ulceration of the affected lymph node occasionally occurs during B. malayi infection, more often than in Bancroftian filariasis. Remnants of adult worms can sometimes be found in the ulcer drainage.[2]
The most obvious sign of infection, elephantiasis, is the enlargement of the limbs–usually the legs. A late complication of infection, elephantiasis is a form of lymphedema and is caused by repeated inflammation of the lymphatic vessels. Repeated inflammatory reactions causes vessel dilation and thickening of the affected lymphatic vessels, which can compromise function. The lymphatic system normally functions to maintain fluid balance between tissues and the blood and serves as an integral part of the immune system. Blockage of these vessels due to inflammatory induced fibrosis, dead worms, or granulomatous reactions can interfere with normal fluid balance, thus leading to swelling in the extremities.[3] Elephantiasis resulting from B. malayi infection typically affects the distal portions of the extremities. Unlike Bancroftian filariasis, B. malayi rarely affects genitalia and does not cause funiculitis, orchitis, epididymitis, hydrocele, or chyluria, conditions more often observed with Bancroftian infection.[2]
Secondary bacterial infection is common among patients with filariasis. Compromised immune function due to lymphatic damage in addition to lymph node ulcerations and abscesses exposure and impaired circulation due to elephantiasis can cause secondary bacterial or fungal infection. Elephantiasis, in addition to the physical burden of a swollen limb, can be a severely debilitating condition given bacterial infection. Part of the WHO's "Strategy to Eliminate Lymphatic Filariasis" targets hygiene promotion programs in order to alleviate the suffering of affected individuals (see Prevention Strategies).[2][4]
However, clinical manifestations of infection are variable and depend on several factors, including host immune system, infectious dose, and parasite strain differences. Most infections appear asymptomatic, yet vary from individual to individual. Individuals living in endemic areas with microfilaremia may never present with overt symptoms, whereas in other cases, only a few worms can exacerbate a severe inflammatory response.[2]
The development of the disease in humans, however, is not well understood. Adults typically develop worse symptoms, given the long exposure time required for infection. Infection may occur during childhood, but the disease appears to take many years to manifest. The incubation period for infection ranges from 1 month to 2 years and typically microfilariae appear before overt symptoms. Lymphedema can develop within six months and development of elephantiasis has been reported within a year of infection among refugees, who are more immunologically naive. Men tend to develop worse symptoms than women.[4]
Hosts of B. malayi include Southeast Asian cats.[5]
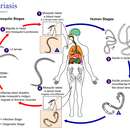
Development and replication of B. malayi occurs in two discrete phases: in the mosquito vector and in the human. Both stages are essential to the life cycle of the parasite.
Mosquito: The mosquito serves as a biological vector and intermediate host – it is required for the developmental cycle and transmission of B. malayi.
4. The mosquito takes a human blood meal and ingests microfilariae (worm-like sheathed eggs) that circulate in the human blood stream.
5-7 In the mosquito, the microfilariae shed sheaths, penetrate the midgut, and migrate to the thoracic muscles were the microfilariae increase in size, molt, and develop into infective larvae (L1 and L3) over a span of 7–21 days. No multiplication or sexual reproduction of microfilariae occurs in the mosquito.
8-1 The infective larvae (L3) migrate to the salivary glands, enter the proboscis and escape onto human skin when the mosquito takes another blood meal.[6]
Human: B. malayi undergoes further development in the human as well as sexual reproduction and egg production.
1-2 The infective larvae (L3) actively penetrate the skin through the bite hole and develop into adults in the lymphatic system over a span of 6 months. Adult worms can survive in the lymphatic system for 5–15 years[7]
3. The male and female adult worms mate and the females produce an average of 10,000 sheathed eggs (microfilaria) daily[7] The microfilariae enter the blood stream and exhibit nocturnal periodicity and subperiodicity.
4. Another mosquito takes a blood meal and ingests the microfilariae. Infection depends on the mosquito taking a blood meal during a periodic episode – when microfilariae are present in the bloodstream.[6]
Adult worms resemble typical nematode roundworms. Long and threadlike, B. malayi and other nematode possess only longitudinal muscles and move in an S-shape motion.[8] Adults are typically smaller than adult W. bancrofti, though few adults have been isolated. Female adult worms (50 mm) are larger than male worms (25 mm).[9]
B. malayi microfilariae are 200–275 µm in length and have a round anterior end and a pointed posterior end. The microfilariae are sheathed, which stains heavily with Giemsa. The sheath is actually the egg shell, a thin layer that surrounds the egg shell as the microfilariae circulates in the bloodstream. The microfilariae retain the sheath until they are digested in the mosquito midgut.[2]
B. malayi microfilariae resemble W. bancrofti and Loa loa microfilariae with minor differences that can aid in laboratory diagnosis. B. malayi microfilariae can be distinguished by the noncontinuous row of nuclei found in the tip of the tail. There are two terminal nuclei that are distinctly separated from the other nuclei in the tail, whereas the tail of W. bancrofti contains no nuclei and Loa loa microfilariae nuclei form a continuous row in the tail. B. malayi microfilariae also have a characteristic cephalic space ratio of 2:1.[10]
B. malayi is transmitted by a mosquito vector. The principal mosquito vectors include Mansonia, Anopheles, and Aedes mosquitoes.[11][2] The geographical distribution of the disease is thus dependent on suitable mosquito breeding habitat.
The accumulation of many infective mosquito bites – several hundreds to thousands – is required to establish infection. This is because a competent mosquito usually transmits only a few infective L3 larvae (see Life cycle), and less than 10% of those larvae progress through all the necessary molting steps and develop into adult worms that can mate.[13] Thus those at greatest risk for infection are individuals living in endemic areas—short term tourists are unlikely to develop lymphatic filariasis.[14]
Tender or enlarged inguinal lymph nodes or swelling in the extremities can alert physicians or public health officials to infection.
With appropriate laboratory equipment, microscopic examination of differential morphological features of microfilariae in stained blood films can aid diagnosis—in particular the examination of the tail portion, the presence of a sheath, and the size of the cephalic space.[2] Giemsa staining will uniquely stain B. malayi sheath pink.[10] However, finding the microfilariae on blood films can be difficult because of the nocturnal periodicity of some forms of B. malayi.
PCR based assays are highly sensitive and can be used to monitor infections both in humans and the mosquito vectors. However, PCR assays are time-consuming, labor-intensive and require laboratory equipment. Lymphatic filariasis mainly affects the poor, who live in areas without such resources.[15]
The ICT antigen card test is widely used in the diagnosis of W. bancrofti, but commercial antigens of B. malayi have not been widely available. However, new research developments have identified a recombinant antigen (BmR1) that is both specific and sensitive in the detection of IgG4 antibodies against B. malayi and B. timori in an enzyme-linked immunosorbent assay and an immunochromatographic rapid dipstick (Brugia Rapid) test. However, it appears that immunoreactivity to this antigen is variable in individuals infected with other filarial nematodes.[16] This research has led to the development of two new rapid immunochromatographic IgG4 cassette tests – WB rapid and PanLF rapid – which detect Bancroftian filariasis and all three species of lymphatic filariasis, respectively, with high sensitivity and selectivity.[15]
There is currently no licensed vaccine to prevent lymphatic filariasis. However, recent research has produced vaccine candidates with good results in experimental animals. A glutathione-S-transferase, a detoxification enzyme in parasites isolated from Setaria cervi, a bovine filarial parasite, reduced B. malayi adult parasite burden by more than 82% for 90 days after treatment.[17]
Vector control has been effective in virtually eliminating lymphatic filariasis in some regions, but vector control combined with chemotherapy produces the best results. It is suggested that 11 to 12 years of effective vector control may eliminate lymphatic filariasis.[18] Successful methods of B. malayi vector control include residual house spraying using DDT and insecticide treated bednets. Mansonia larvae attach their breathing tubes to underwater roots and plants in order to survive. While chemical larvicides have only provided partial control, plant removal could prevent vector development, but also potential adverse effects on the aquatic environment. Lymphatic filariasis vector control is neglected in comparison to the far more established efforts to control malaria and dengue vectors. Integrated vector control methods should be applied in areas where the same mosquito species is responsible for transmitting multiple pathogens.[19]
The Global Alliance to Eliminate Lymphatic Filariasis was launched by the World Health Organization in 2000 with two primary goals: 1) to interrupt transmission and 2) to alleviate the suffering of affected individuals. Mass drug treatment programs are the main strategy for interrupting parasite transmission, and morbidity management, focusing on hygiene, improves the quality of life of infected individuals.[20]
A goal of community-based efforts is to eliminate microfilariae from the blood of infected individuals in order to prevent transmission to the mosquito. This is primarily accomplished through the use of drugs. The treatment for B. malayi infection is the same as for Bancroftian filariasis. Diethylcarbamazine has been used in mass treatment programs as an effective microfilaricidal drug in several locations, including India.[21] While diethylcarbamazine tends to cause adverse reactions like immediate fever and weakness, it is not known to cause any long-term adverse drug effects. It has been shown to kill both adult worms and microfilariae. In Malaysia, diethylcarbamazine dosages (6 mg/kg weekly for 6 weeks; 6 mg/kg daily for 9 days) reduced microfilariae by 80% for 18–24 months after treatment in the absence of mosquito control.[2] Microfilariae numbers slowly return many months after treatment, thus requiring multiple drug doses over time in order to achieve long-term control. However, it is not known how many years of mass drug administration is required to eliminate transmission. there have been any confirmed cases of diethylcarbamazine resistance as of 2007.[21]
Single doses of two drugs (albendazole-diethylcarbamazine and albendazole-ivermectin) have been shown to remove 99% of microfilariae for a year after treatment and help to improve elephantiasis during early stages of the disease.[20] Ivermectin does not appear to kill adult worms but serves as a less toxic microfilaricide.[2]
Since the discovery of the importance of Wolbachia bacteria in the life cycle of B. malayi and other nematodes, novel drug efforts have targeted the endobacterium. Tetracyclines, rifampicin, and chloramphenicol have been effective in vitro by interfering with larvae molting and microfilariae development. Tetracyclines have been shown to cause reproductive and embryogenesis abnormalities in the adult worms, resulting in worm sterility. Clinical trials have demonstrated the successful reduction of Wolbachia and microfilariae in onchocerciasis and W. bancrofti infected patients. These antibiotics, while acting through a slightly more indirect route, are promising antifilarial drugs.[22]
Secondary bacterial infection is often observed with lymphatic filariasis. Rigorous hygiene practices, including washing with soap and water daily and disinfecting wounds can help heal infected surfaces, and slow and potentially reverse existing tissue damage. Promoting hygiene is essential for lymphatic filariasis patients given the compromised immune and damaged lymphatic systems and can help prevent suffering and disability.[14][20]
B. malayi infects 13 million people in south and southeast Asia and is responsible for nearly 10% of the world's total cases of lymphatic filariasis.[18][19] B. malayi infection is endemic or potentially endemic in 16 countries, where it is most common in southern China and India, but it also occurs in Indonesia, Thailand, Vietnam, Malaysia, the Philippines, and South Korea.[11] The distribution of B. malayi overlaps with W. bancrofti in these regions, but does not coexist with B. timori.[2] Regional foci of endemicity are determined in part by the mosquito vectors
B. malayi was discovered in 1927 by the Dutch parasitologist Steffen Lambert Brug (1879–1946) (who is commonly known in the scientific literature as S.L. Brug) while working in Indonesia. It was similar to another filarial roundworm Wuchereria bancrofti (then called Filaria (Microfilaria) bancrofti). But the new species of human filaria in North Sumatra was both physiologically and morphologically distinct from the W. bancrofti microfilariae commonly found in Jakarta. Based on their resemblance and differences, the new species was named Filaria malayi.[23] Despite epidemiological studies identifying Filaria malayi in India, Sri Lanka, China, North Vietnam, and Malaysia in the 1930s, Lichtenstein and Brug's hypothesis was not accepted until the 1940s, when Rao and Mapelstone identified two adult worms in India.[24]
Based on the similarities with W. bancrofti, Rao and Mapelstone proposed to call the parasite Wuchereria malayi.[23] After the discovery of new species such as W. pahangi (now B. pahangi) in 1956, and W. patei (now B. patei) in 1958, the scientific classification was reassessed in 1960. Buckley proposed to divide the old genus Wuchereria, into two genera, Wuchereria and introduced a new Brugia after the original discoverer. Then Wuchereria contains only W. bancrofti, which so far has been found to infect only humans, and the genus Brugia contains B. malayi, which infects humans and animals, as well as other zoonotic species.[12]
In 1957, two subspecies of human infecting B. malayi were discovered by Turner and Edeson in Malaysia based on the observation of different patterns of microfilaria periodicity.[23] Periodicity refers to a pronounced peak in microfilariae count during a 24‑hour interval when microfilariae are present and detectable in the circulating blood.[12] The basis for this phenomenon remains largely unknown.[2]
In 2007, scientists sequenced the genome of Brugia malayi.[25] Identifying the genes of this organism might lead to development of new drugs and vaccines.[26]
To decipher the genome, "Whole Genome Shotgun Sequencing" was performed. The genome was found to be approximately 90-95 megabases in size. The results of the sequencing were then compared to those of the reference nematode Caenorhabditis elegans, along with its prototype Caenorhabditis briggsae. These two free-living nematodes were incorporated in the study and were important for several reasons:
Sequence comparisons between the two genomes allow for mapping of C. elegans orthologs to B. malayi genes. By using orthology mappings (between C. elegans and B.malayi) and incorporating the extensive genomic and functional genomic data, including genome-wide RNAi screens that already exist for C. elegans, potentially essential genes in B. malayi can be identified. Scientists are hoping to be able to target these genes as potential new targets for drug treatments. The longevity of this parasite complicates treatment because most existing drugs target the larvae and thus do not kill adult worms. The drugs often must be taken periodically for years, and the worms can cause a massive immune reaction when they die and releases foreign molecules in the body. Drug treatments for filariasis have not changed significantly in over 20 years, and with the risk of resistance rising, there is an urgent need for the development of new anti-filarial drug therapies. From the genome sequence, several metabolic pathways have been identified, containing dozens of gene products that may be helpful in the discovery of more targeted and effective drug therapies.
These potential new targets for drugs or vaccines may provide new opportunities for understanding, treating and preventing elephantiasis.
The relationship between the Wolbachia bacteria and B. malayi is not fully understood. Extrapolating from research done with Wuchereria bancrofti, another nematode that causes filariasis, Wolbachia may aid in embryogenesis of the worm, be responsible for potent inflammatory responses from macrophages and filarial disease, and be linked to the onset of lymphedema and blindness sometimes associated with B. malayi infections. In a study done by the University of Bonn in Ghana, doxycycline effectively depleted Wolbachia from W. bancrofti. It is likely that the mechanism of doxycycline is similar to that in other filarial species, i.e., a predominant blockade of embryogenesis, leading to a decline of microfilariae according to their half-life. This could render doxycycline treatment an additional tool for the treatment of microfilaria-associated diseases in Bancroftian filariasis, along with B. malayi fiariasis. The course of treatment with doxycycline could be much shorter as it would make the adult worm sterile in one shot rather than repeatedly have to target the replenished larvae that current treatments kill, and there would be fewer side effects for the infected individual.
Another hopeful use for the research is in the area of transplant research. Because the B. malayi genome is the first parasitic genome to have been sequenced, the implications on the mechanism of parasitism in humans are crucial to understand. According to Alan L. Scott, Ph.D., a collaborator at Johns Hopkins University, understanding how a particular parasite, such as B. malayi, can adapt to humans, may yield medical benefits far beyond treating elephantiasis. According to the author, "This worm can reside in the host for years and not necessarily cause disease, in fact the less disease the individual has, the more worms there are in circulation. Now that we know those genes don't exist in humans we can target them to control disease." Some of the predicted proteins for these new genes appear similar to known immuno-modulator proteins, regulators of the immune system, suggesting that they are involved in deactivating the host's immune system to ensure the parasite remains undetected. Knowledge of these previously unknown immune suppressors could also be of use in organ transplants and to help treat autoimmune disease.
According to the Filarial Genome Project being done by The Special Programme for Research and Training in Tropical Diseases, the Brugia malayi MIF gene is expressed in all life-cycle stages of the parasite, and results suggest that B. malayi MIF may interact with the human immune system during the course of infection by altering the function of macrophages in the infected individual. Studies are currently testing the hypothesis that MIF may be involved in reducing the host's immune response to the microfilariae. Understanding how this particular parasite has adapted to humans may help organ transplant researchers by figuring out how to prevent the immune system from attacking the transplanted tissue.
Brugia malayi is a filarial (arthropod-borne) nematode (roundworm), one of the three causative agents of lymphatic filariasis in humans. Lymphatic filariasis, also known as elephantiasis, is a condition characterized by swelling of the lower limbs. The two other filarial causes of lymphatic filariasis are Wuchereria bancrofti and Brugia timori, which both differ from B. malayi morphologically, symptomatically, and in geographical extent.
B. malayi is transmitted by Mansonia mosquitoes and is restricted to South and Southeast Asia. It is one of the tropical diseases targeted for elimination by the year 2020 by the World Health Organization, which has spurred vaccine and drug development, as well as new methods of vector control.
Brugia malayi es un especie de nematodo espirúrido que causa filariasis en humanos.[1] Identificado por Lichtenstein y nombrado por Brug en 1927, diferenciándolo de la especie Wuchereria bancrofti, llamado inicialmente Filaria malayi. En 1958 el nuevo género Brugia fue propuesto por Buckley, y el cambio produjo la especie Brugia malayi. Es un organismo limitado a las regiones tropicales de Asia. Son transmitidos al hombre por mosquitos, en especial Mansonia, Anopheles y Aedes.
Las larvas infectantes son transmitidas en la picadura de artrópodos infestados. Las larvas migran al sitio apropiado del cuerpo del hospedador, donde se desarrollan en adultos productores de microfilarias. Los adultos se alojan en varios tejidos humanos donde pueden vivir durante varios años. Los agentes de la filariasis linfática residen en los vasos y ganglios linfáticos. B. malayi tiende a alojarse particularmente en los vasos linfáticos, tal como Wuchereria bancrofti. Los gusanos hembras producen microfilarias, que circulan en la sangre.
Las microfilarias infectan mosquitos, dentro del cual se desarrollan en 1 o 2 semanas en una larva filariforme (3.er estadio) infectante. Durante las subsecuentes picadas del insecto, las larvas infectan el hospedador vertebrado. Migran a los vasos linfáticos, donde se desarrollan en adultos, un proceso lento que puede requerir hasta 18 meses.
Recientemente se descubrió que B. malayi contiene una bacteria endosimbiótica, Wolbachia, en todos sus estadios de vida.[2] La secuencia genómica de esta bacteria se determinó en los Estados Unidos, indicando también que Wolbachia puede ser destruida al tratar el hospedador humano con doxiciclina. Los nematodos curados de la bacteria son infértiles y gozan de una incrementada motilidad. la enfermedad que trasmite este parásito se llama filariasis malaya
Las microfilarias miden 270 por 8 µm, tienen una vaina que recubre su cuerpo y una cola con una constricción terminal, núcleos elongados pero ausentes en la porción cefálica. La vaina que cubre al organismo se colorea cuando el preparado microscópico se tiñe, a diferencia de Wuchereria bancrofti, el cual no retiene el colorante.[3]
Brugia malayi es un especie de nematodo espirúrido que causa filariasis en humanos. Identificado por Lichtenstein y nombrado por Brug en 1927, diferenciándolo de la especie Wuchereria bancrofti, llamado inicialmente Filaria malayi. En 1958 el nuevo género Brugia fue propuesto por Buckley, y el cambio produjo la especie Brugia malayi. Es un organismo limitado a las regiones tropicales de Asia. Son transmitidos al hombre por mosquitos, en especial Mansonia, Anopheles y Aedes.
La filaire de Malaisie (Brugia malayi) est une espèce de nématodes de la famille des Onchocercidae. c'est un ver filiforme dont la présence dans les ganglions mésentériques entraîne la filariose de Malaisie ou filariose lymphatique orientale. Cette espèce appartient au genre Brugia, qui regroupe des nématodes non segmentés, recouverts d'une épaisse cuticule et menant une vie libre ou parasitaire.
Comme les autres filaires, la filaire de Malaisie est ovovivipare. Elle ne pond pas d'œufs mais des larves appelées microfilaires circulant dans le sang. Les adultes, appelés macrophilaires, vivent dans la circulation lymphatique.
Les adultes ne se différencient pas de ceux de la filaire de Bancroft.
En revanche, les larves se distinguent par des dimensions légèrement plus petites (200 à 240 μm), un espace céphalique un peu plus long (6 μm) et deux renflements (sub-terminal et terminal) de l'extrémité caudale. La coloration au Giemsa du corps interne donne un vermillon divisé en 3 masses contre un vermillon unique pour la filaire de Bancroft[1].
Les hôtes intermédiaires et vecteurs sont des moustiques généralement Mansonia, mais aussi Culex, Aedes, Anopheles selon la région. Les moustiques du genre Mansonia sont très anthropophiles (piquant préférentiellement l'homme) mais aussi exophiles (ne piquant qu'à l'extérieur des habitations).
Le vecteur principal (moustique Mansonia) se développe dans les mares et marécages ouverts (M. uniformis, M. annulifera, M. indiana) ou dans les forêts inondées bordant les cours inférieurs des fleuves (M. dives, M. bonneæ, M.annulata). Le premier groupe, celui des mares, est quasi-exclusivement anthropophile, alors que le second, celui des forêts, est aussi zoophile (outre l'homme, les singes et les carnivores).
Les microfilaires sont à périodicité nocturne[2] moins constante que celles de Wuchereria bancrofti (filaire de Bancroft), elles sont semi-nocturnes ou apériodiques (pas de périodicité particulière), ce qui est en rapport avec la diversité des vecteurs locaux (différentes heures d'activité)[1]. Toutefois leur évolution et leur transmission sont semblables.
Ici encore, les adultes vivent dans le système lymphatique, mais surtout dans les ganglions mésentériques.
Le génome de Brugia malayi est entièrement séquencé[3] et les informations relatives sont compilées dans WormBase.
Purement asiatique, cette filaire se rencontre dans un vaste triangle, allant de l'ouest de l'Inde à la Corée et au sud de l'Indonésie, où elle pose, sur le plan de la prophylaxie, de nombreuses difficultés :
C'est également une filariose (helminthiase) lymphatique, mais avec ses caractères propres
Il existe d'abord des adénopathies situées au cou, à l'aisselle, au coude, ou à l'aine. Elles sont superficielles, mobiles, molles et indolores. Elles peuvent se compliquer de crises de lymphangite siégeant surtout aux bras. On observe souvent des signes pulmonaires (toux, dypsnée à type d'asthme)[1].
L'examen de sang peut révéler, en plus de l'éosinophilie élevée, une hyperleucocytose très marquée, allant de 15 000 à presque 50 000 éléments par mm³.
L'évolution se fait par poussées, vers l'éléphantiasis, augmentation considérable du volume d'un membre ou d'une partie du corps, causée par un œdème dur et chronique des téguments. Celui de la filaire de Malaisie respecte le plus souvent les zones génitales. Il se localise presque uniquement au membre inférieur, au-dessous du genou, réalisant la classique « jambe de Cochin[4] » ; ou alors à l'avant-bras. Ces éléphantiasis sont toujours moins importants que ceux qui peuvent être provoqués par la filaire de Bancroft[1].
L'évolution peut être favorable si l'on soustrait le malade suffisamment tôt aux ré-infestations constantes des zones d'endémie. Sinon l'évolution est capricieuse, d'autant plus défavorable qu'elle a débuté précocement dans la vie du sujet. Des périodes de stabilisation alternent avec des aggravations liées à des infections. La sédentarité liée au handicap augmentent les risques de lésions cardiaques et rénales[1].
Il se fera classiquement par la recherche des microfilaires dans le sang périphérique prélevé selon la périodicité. Ce diagnostic est difficile, car les microfilaires sont souvent très peu nombreuses dans le sang.
La preuve formelle peut être apportée dans le liquide de ponction ganglionnaire ; ou dans la biopsie ganglionnaire, par macération d'une partie dans du liquide physiologique et centrifugation, par examen histologique du reste.
Le traitement sera le même que pour la filariose de Bancrofti. (Voir Wuchereria bancrofti).
Il est particulièrement sensible à un traitement antibiotique (doxycycline) qui va éliminer le symbionte bactérien dont il dépend.
La filaire de Malaisie (Brugia malayi) est une espèce de nématodes de la famille des Onchocercidae. c'est un ver filiforme dont la présence dans les ganglions mésentériques entraîne la filariose de Malaisie ou filariose lymphatique orientale. Cette espèce appartient au genre Brugia, qui regroupe des nématodes non segmentés, recouverts d'une épaisse cuticule et menant une vie libre ou parasitaire.
Comme les autres filaires, la filaire de Malaisie est ovovivipare. Elle ne pond pas d'œufs mais des larves appelées microfilaires circulant dans le sang. Les adultes, appelés macrophilaires, vivent dans la circulation lymphatique.
Brugia malayi Brug, 1927 è un nematode parassita dell'uomo, una delle tre specie appartenenti alla famiglia Onchocercidae che causa la filariasi linfatica, altrimenti detta "elefantiasi", malattia caratterizzata dal diffuso gonfiore degli arti inferiori. Gli altri due vermi filariali che causano identica malattia sono il Wuchereria bancrofti e il Brugia timori, che differiscono dal B. malayi morfologicamente, nei sintomi indotti all'ospite e nelle regioni in cui sono attive le infezioni.[1]
I vettori di questo parassita sono alcuni tipi di zanzare distribuite in alcune zone del sud e del sudest asiatico. È una delle malattie tropicali che l'Organizzazione mondiale della sanità si prefigge di debellare entro il 2020, grazie allo sviluppo di un vaccino e farmaci specifici, oltre che nuovi metodi per contrastare i vettori del parassita.
Lichentenstein e Brug identificarono per la prima volta il B. malayi come agente patogeno distinto nel 1927. Riportarono all'epoca di un nematode parassita dell'uomo nella zona nord di Sumatra che era fisiologicamente e morfologicamente differente dal W. bancrofiti comunemente presente a Giacarta, e chiamarono questa nuova specie Filaria malayi.[2] Malgrado gli studi epidemiologici che identificarono il nuovo nematode in India, Sri Lanka, Cina, Vietnam del Nord e Malaysia, la scoperta dei due biologi non fu accettata fino al 1940, con l'identificazione di due vermi adulti in India da parte dei biologi Rao e Mapelstone.[3]
Per la somiglianza con il W. bancrofiti Rao e Mapelstone proposero di chiamare la nuova specie Wuchereria malayi[2], ma nel 1960 fu proposto di dividere il vecchio genere Wuchereria creandone uno nuovo, il Brugia, rinominando così la nuova specie Brugia malayi. Mentre i parassiti del genere Wuchereria sono in grado di infettare unicamente gli esseri umani, i Brugia hanno invece la capacità di infettare diverse specie oltre l'uomo.[4]
Nel 1957 furono scoperte due sottospecie di B. malayi in Malesia, basandosi sull'osservazione di differenti modelli dello stadio larvale periodico del parassita (microfilaria).[5] La differenza di periodicità tra le due specie si riferisce al ciclo di 24 ore nelle quali le microfilarie sono rilevabili con diversa densità nel sangue,[4] e le cause di questo fenomeno rimangono tuttora sconosciute.[6]
I vettori di questo parassita sono alcune zanzare del genere Mansonia, Anopheles e Aedes.[6][7] La presenza delle infezioni causate dal B. malayi dipende quindi dalle condizioni favorevoli allo sviluppo di queste zanzare.
L'infezione si contrae nel tempo dopo centinaia o migliaia di morsicature da parte di zanzare infette, questo perché normalmente ad ogni morso vengono trasmesse un numero limitato di larve mature (stadio L3), e solo un 10% di queste riescono a evolversi in vermi adulti.[8] I soggetti che corrono il rischio di contrarre l'infezione sono dunque quelli che vivono abitualmente nelle zone endemiche, mentre il rischio per un turista di passaggio che dovesse trascorrere poco tempo in un'area a rischio avrebbe poche probabilità di essere infettato.[9]
Lo sviluppo e la riproduzione del parassita avviene in due fasi distinte: nella zanzara (il vettore) e nell'uomo (l'ospite). Entrambe le fasi sono imprescindibili per il ciclo vitale del nematode, che altrimenti non potrà svilupparsi in un verme adulto.
Fase di sviluppo nella zanzara: La zanzare funge da vettore e ospite intermedio, è essenziale nel primo sviluppo larvale del parassita e nella sua trasmissione.
4.La zanzara si ciba del sangue umano da un soggetto infetto e preleva da questo i microfilaria (uova filiformi del nematode) che circolano nel flusso sanguigno.
5-7Nella zanzara i microfilaria penetrano nell'intestino e successivamente migrano verso i muscoli del volo, dove iniziano a crescere per poi svilupparsi in larve, in un periodo che va dai 7 ai 21 giorni. All'interno della zanzara non avviene alcuna riproduzione sessuale dei parassiti.
8-1Le larve dal potenziale infettante (stadio larvale L3 migrano verso la ghiandola salivare, dalla quale fuoriescono nel momento in cui la zanzara si ciba nuovamente di sangue umano infettando l'ospite.[10]
Fase di sviluppo nell'uomo: Il parassita si sviluppa completamente nel corpo umano, dove si riproduce sessualmente e depone le uova.
1-2Le larve infettanti penetrano attivamente sotto la pelle attraverso il foro creato dal morso della zanzara e si sviluppano in vermi adulti nel sistema linfatico in un periodo di circa 6 mesi. Gli adulti possono vivere nel sistema linfatico dai 5 ai 15 anni[11]
3.I maschi e le femmine adulti si accoppiano, e la femmina produce giornalmente una media di 10.000 microfilarie al giorno.[11] Le microfilarie entrano dunque nel flusso sanguigno, mostrando alle analisi la classica periodicità a seconda del tipo di infezione contratta.
4.Un'altra zanzara si ciba del sangue dell'ospite infettato ingerendo nuovamente le microfilarie riprendendo il ciclo. Il prelievo delle uova dipende dal tipo di infezione, ovvero se nel momento in cui la zanzara morde l'ospite sono presenti o meno le microfilarie nel flusso sanguigno.[6][10]
Gli esemplari adulti sono simili ai classici nematodi, lunghi e filiformi, come le altre specie possiedono unicamente muscoli longitudinali e si muovono attraverso un movimento a "S" del corpo.[12] Gli adulti sono generalmente più piccoli del W. bancrofti, anche se il dato non è completo poiché il numero di esemplari isolati finora è esiguo. Le femmine adulte sono larghe il doppio rispetto ai maschi, mentre le prime hanno in media una circonferenza di 50 mm, il dato nei maschi è di 25 mm.[13]
Le uova del B. malayi misurano tra i 200 e i 275 μm di lunghezza ed hanno l'estremità anteriore arrotondata e l'estremità anteriore appuntita. Il rivestimento di cui sono coperte viene rilevato tramite la colorazione di Giemsa, che ne indica quindi la presenza nel sangue. Questo rivestimento è in sostanza il guscio dell'uovo, che circonda la larva mentre questa circola nel sangue. Il rivestimento rimane integro finché i microfilaria non vengono ingeriti dalle zanzare nell'intestino.[6] I microfilaria di questo parassita sono molto simili a quelli del W. bancrofti e il Loa loa, ma le piccole differenze possono aiutare nell'identificazione dagli esami in laboratorio. Tra le differenze vi è una discontinuità del nucleo sulla punta della coda, laddove le uova del W. bancrofti non contiene affatto un nucleo e nel Loa loa il nucleo forma invece un filo continuo nella coda.[6][14]
B. malayi è uno dei parassiti responsabili della filariasi linfatica, caratterizzata dall'infezione e gonfiore del sistema linfatico. La malattia è causata dalla presenza dei vermi nel sistema linfatico e la risposta dell'organismo ospite. I segni dell'infezione sono identici a quelli causati dal W. bancrofti, ovvero linfoadenopatia, linfedema e linfangite, oltre a infezioni batteriche collaterali, molto comuni.
La linfoadenopatia, il gonfiore dei linfonodi, è un sintomo comune di molte malattie. Nelle prime manifestazioni della filariasi, la linfoadenopatia si manifesta spesso nella zona inguinale quando questa è causata dal B. malayi, e può insorgere prima della maturazione dei vermi.[6]
La linfangite è l'infiammazione dell'apparato circolatorio linfatico in risposta all'infezione. Si manifesta inizialmente in risposta allo sviluppo dei vermi, alla muta, la morte o per infezioni batteriche e fungine. Il sistema colpito diventa teso e morbido, e la pelle sovrastante presenta eritemi e diventa calda. In alcuni casi l'infezione da B. malayi forma ascessi e ulcerazioni dei linfonodi colpiti, in percentuale maggiore rispetto alla filariasi causata dal W. bancrofti. Durante il drenaggio delle ulcere possono essere rinvenuti i resti di vermi adulti.[6]
Il segno più evidente dell'infezione, l'elefantiasi, è l'ingrossamento a dismisura degli arti. Rappresenta un sintomo dell'infezione in stato avanzato, ed è un linfedema causato dalla continua infiammazione del sistema circolatorio linfatico. Ripetute infiammazioni causano l'allargamento e il restringimento del sistema affetto, compromettendone la funzionalità. Il sistema linfatico normalmente mantiene bilanciati i fluidi tra il sangue e i tessuti, ed è parte integrante del sistema immunitario. Il blocco della circolazione nei linfonodi causato dalla presenza di vermi morti e le fibrosi possono interferire con il normale bilanciamento dei fluidi, portando dunque al gonfiore delle estremità.[15] L'elefantiasi causata dal B. moryi affligge tipicamente la zona degli arti inferiori sotto il ginocchio. Diversamente dalle filariasi bancroftiane, il B. malayi colpisce raramente i genitali, e non causa orchiti e altri sintomi invalidanti spesso osservati con le infezioni causate dal W. bancrofti.[6]
Le infezioni batteriche secondarie sono molto comuni nei pazienti affetti da filariasi. Il sistema immunitario compromesso a causa del danno linfatico, unito agli ascessi e le ulcerazioni dei linfonodi e la circolazione resa difficile dall'elefantiasi pongono condizioni favorevoli al proliferare di funghi e batteri. Una delle strategie per alleviare le sofferenze di chi è affetto da queste infezioni è di promuovere programmi di igiene per prevenire le infezioni batteriche e fungine.[6][16]
In ogni caso, le manifestazioni cliniche sono molto variabili e dipendono da diversi fattori, come lo stato del sistema immunitario dell'ospite prima dell'infezione, il livello di infestazione e il ceppo del parassita. Molte infezioni sono asintomatiche, ma variano spesso da individuo a individuo. Gli individui che vivono nelle zone endemiche del parassita possono anche non presentare sintomi, mentre in alcuni casi pochi vermi adulti nell'organismo possono dare luogo ad una seria risposta infiammatoria.[6] Lo sviluppo della malattia nell'uomo comunque non è ancora ben compreso. Gli adulti generalmente sviluppano i sintomi peggiori, a causa della lunga esposizione al parassita necessaria per lo sviluppo della malattia. L'infezione può colpire durante l'infanzia, ma per svilupparsi necessita di anni. Il periodo di incubazione varia da un mese a due anni, e normalmente le microfilarie vengono trovate nella circolazione sanguigna prima che possano presentarsi sintomi. Il linfedema può svilupparsi in sei mesi, mentre l'elefantiasi vera e propria può presentarsi anche dopo un solo anno dall'infezione in soggetti immunodepressi. Gli uomini sviluppano sintomi con maggiore gravità rispetto alle donne.[16]
Brugia malayi Brug, 1927 è un nematode parassita dell'uomo, una delle tre specie appartenenti alla famiglia Onchocercidae che causa la filariasi linfatica, altrimenti detta "elefantiasi", malattia caratterizzata dal diffuso gonfiore degli arti inferiori. Gli altri due vermi filariali che causano identica malattia sono il Wuchereria bancrofti e il Brugia timori, che differiscono dal B. malayi morfologicamente, nei sintomi indotti all'ospite e nelle regioni in cui sono attive le infezioni.
I vettori di questo parassita sono alcuni tipi di zanzare distribuite in alcune zone del sud e del sudest asiatico. È una delle malattie tropicali che l'Organizzazione mondiale della sanità si prefigge di debellare entro il 2020, grazie allo sviluppo di un vaccino e farmaci specifici, oltre che nuovi metodi per contrastare i vettori del parassita.
Brugia malayi é uma espécie de nematódeo da família Onchocercidae. São parasitos de mamíferos, incluindo os humanos, causando a dirofilariose linfática.[1]
Brugia malayi é uma espécie de nematódeo da família Onchocercidae. São parasitos de mamíferos, incluindo os humanos, causando a dirofilariose linfática.


